Executive summary
The Strategy for people with Physical Disability and Sensory Impairment (PDSI) confirms the Surrey County Council Adult Social Care commitment to improving outcomes, services, and support for disabled adults. It was co-produced with the support of Surrey Coalition for Disabled People during June 2021 to April 2022.
The strategy looks at how support needs to change and develop to facilitate disabled people to fulfil their aspirations. An important part of the co-production was to learn lessons from what works well and explore how this can be built on, and to identify gaps and/or changes in support required. Making changes at a local level will demand a culture shift across all sectors - statutory, voluntary, community and commercial.
The strategy identifies priorities to deliver the vision of services that people with physical and/or sensory impairment want and makes commitments as to action the council will take to address them. The 6 key themes are:
- community inclusion – relating to support and facilities and facilitating welcoming and accessible neighbourhoods, communities, and employers
- establish an effective approach to securing improved accommodation: new housing options, access to aids and adaptations, access to social housing
- ensure our direct payments offer acts as a constructive way to maximize choice, control and independence
- establish workforce development initiatives that support practitioners to work in partnership with people regarding their support and reflect best practice
- ensure carers of disabled people have access to the support they need and recognise them as expert partners in care
- partnership work with NHS colleagues to improve care pathways and achieve better health outcomes for residents
In addition, the strategy also demonstrates our commitment to establishing a new governance structure, co-produced with disabled people, and the development of an indicator set and dashboard to monitor our progress.
To support the market development needed for effective delivery of the strategy we will co-produce a market position statement.
Finally, we will hold an annual event to support the engagement of the whole system to review progress and refresh the delivery plan.
Throughout the lifespan of the strategy, we will continue to work with people with a wide range of physical and/or sensory impairment to ensure that they continue to shape services and benefit from improved outcomes.
Please note: Most of the data and messages presented in the strategy relate to people aged 18 to 64 years, though we recognise that older people, people with mental health problems and people with learning disabilities will access services that people with physical disabilities and/or sensory impairments use.
Introduction
This strategy covers people with physical disabilities and sensory impairments. It covers people who are aged 18+. It should be read in conjunction with other strategies which provide more detail in certain areas, for example:
- Accommodation with Care and Support Strategy
- emerging Direct Payments Strategy
- Older People's Strategy
- commissioning strategies for people with learning disabilities and/or autism and people with mental health needs
This strategy:
- sets out what we know about the needs of people with physical disabilities and sensory impairments generally, and in Surrey
- develops and articulates a shared understanding, vision, and action plan of how we will respond to the needs of people with physical disabilities and sensory impairments. Some needs are unique to disabled people, and some of them are universal issues that are exacerbated by one's disability
This strategy is for the next 5 years, 2022 to 2027. As such it does not contain the detail of how the strategy's vision will be achieved. A Strategy Action Plan will be developed setting out how the actions will be achieved. Much of this action planning will be done with the established user forums, in conjunction with Surrey Coalition of Disabled People, and other key partners.
"Sometimes I think the public perception of disability is very poor and expectations are very low". (User participant at Disability Empowerment Network (DENS), 2021)
Throughout the strategy and action plan where the terms "people who are disabled" or "people with disabilities" are referred to, this should be interpreted as including people with a physical, communication, general, sensory and / or neuro-disability including acquired brain injury.
The term "neuro-disability" includes the range of conditions such as Acquired Brain Injury, Multiple Sclerosis, Parkinson's Disease and congenital and childhood conditions such as Cerebral Palsy, Muscular Dystrophy and Spina-Bifida and other rare conditions such as Motor Neurone Disease, Huntington's Disease and Progressive Supra-nuclear Palsy.
A person is considered disabled if they have a self-reported long-standing illness, condition or impairment, which causes difficulty with day-to-day activities. This definition is consistent with the Equality Act 2010 and the Government Statistical Service (GSS) harmonised definition.
Section 1. Vision and values
Contents
- Vision and values
- 1.1 The social model of disability
- 1.2 Commitment to co-production
- 1.3 Objectives of the strategy
Surrey Community Vision 2030
We want Surrey to be a uniquely special place where everyone has a great start in life, people live healthy and fulfilling lives, are enabled to achieve their full potential and contribute to their community and where no one is left behind.
Adult Social Care Vision
To promote people's independence and wellbeing, through personalised care and support that focuses upon their strengths, the outcomes they want to achieve and enables choice and control.
We want Surrey to be a place that offers opportunities for people to live healthy and fulfilling lives, where people's contributions to their local communities are welcomed, supported and valued, and no one is left behind. These opportunities should extend to all disabled people in Surrey. All organisations involved in developing and implementing this strategy are committed to ensuring that the vision and aims will be delivered in full for disabled people.
The vision for this strategy is that, by the end of its life (2022 to 2027), the services commissioned and provided by health and social care organisations for people who are disabled will have developed in such a way that they:
- support people with disabilities to become well informed and expert in their own needs and better able to exercise their rights, choices and life opportunities
- promote health, wellbeing and maximise potential of individuals
- encourage the social inclusion of people with disabilities and work to address the stigma associated with disability
- encourage family and person-centred services and the promotion of independent living options
- Aare tailored to meet the changing needs of people over the course of their lifetime
- continue to promote and enable balanced risk taking
Why do we need a strategy?
People with disabilities have told us that there are significant barriers to achieving our vision across the service system and the wider community. Addressing these barriers will require better understanding of disabilities, and culture change across Surrey's workforce, services and community.
The work of the strategy will need to be embedded in organisations and the wider community so that it is sustained and can be built on. The strategy is here to focus the action of all the partners across Surrey who will work together to make the changes we need to see.
1.1 The social model of disability
The social model of disability is a way of viewing the world, developed by disabled people. This strategy is based on this model of disability.
The model says that people are disabled by barriers in society, not by their impairment or difference. Barriers can be physical, like buildings not having accessible toilets. Or they can be caused by people's attitudes to difference, like assuming disabled people can't do certain things.
The social model helps us recognise barriers that make life harder for disabled people. Removing these barriers creates equality and offers disabled people more independence, choice, and control.
1.2 Commitment to co-production
Co-production is an approach to decision-making and service design rather than a specific method. It stems from the recognition that if organisations are to deliver successful services, they must understand the needs of their users and engage them closely in the design and delivery of those services.
Co-production rejects the traditional understanding of service users as dependents of public services, and instead redefines the service/ user relationship as one of co-dependency and collaboration. Just like users need the support from public services, so service providers need the insights and expertise of its users in order to make the right decisions and build effective services.
1.3 Objectives of the strategy
The objectives of the strategy are to:
- Support people with disabilities to better exercise their rights, choices and life opportunities by:
- working with partners to develop inclusive communities across Surrey
- working with community leads (for example in the voluntary, business and sectors) to identify barriers to inclusion and create solutions that make the most of opportunities to improve services
- working with strategic leads and partners to improve access to housing, employment, and financial advice and services
- supporting young adults to transition to adult services and sources of support
- developing and maintaining a dynamic website of the support available, who from, and how to access it
- doing more locally to make technology more accessible, improve digital literacy, and reduce digital exclusion
- continuing to support user-led organisations and forums, and work with disabled people, so that we understand the issues properly and find solutions that work
- Support the continuing development of an inclusive and effective range of high-quality health and social care services. Initiatives will include:
- the development of a market position statement
- the development of care at home offer
- the development of appropriate accommodation with care and support
- ensuring the development of the direct payments offer considers the needs of people with physical disabilities and sensory impairments
- Develop a more integrated approach to the planning and management of services within and across Surrey County Council and the independent, community, faith, and voluntary sectors, and in the first year of the Strategy, seek to develop partnerships with health care services to enable effective and smoother care pathways
- Ensure that an appropriate implementation infrastructure is put in place to oversee performance and delivery of the strategy by:
- establishing a governance structure that embeds co-production with service users, their families, providers, and practitioners
- establishing a performance dashboard
- developing clear and achievable actions, and recommendations for their implementation, that are monitored and evaluated throughout the life of the strategy
Section 2. Prevalence data, Surrey County Council expenditure on care and support
Contents
- 2.1 Living with a disability
- 2.2 Surrey context
- 2.3 Living with sight loss
- 2.4 Living with hearing loss
- 2.5 Living with a long-term neurological condition (LTNC)
- 2.6 Surrey County Council's expenditure on care and support (2020)
This section sets out the high-level national prevalence data for people disabilities and/or sensory impairments, provides some Surrey specific data, and sets out the key areas of expenditure on care and support services.
Estimating the numbers of disabled people is not easy because there are different ways of defining disability. For example, some definitions are so all encompassing they are likely to provide over-estimates. At the same time, definitions which rest on clinically diagnosed disabilities can provide underestimates of those people who experience difficulties in everyday life due to a physical or other impairment. As a result, there are multiple reasons for the differences in prevalence data. Much of this variation arises from differences in the definitions of disability being used, the age range of the populations to which they apply (like working age, all adults or total population), or differences in how definitions are used.
We recognise the need to improve our data collection locally, so we have clarity regarding the prevalence rates of disability in Surrey, and how they might compare to national data. Strengthening our data collection will help improve our responsiveness and performance, recognising that disability is a complex experience that benefits from a multidisciplinary approach to develop effective actions and policy.
We will: Co-produce a performance dashboard as part of the infrastructure to implement change, initially overseen and regularly reviewed by the Physical Disability and Sensory Impairment Steering Group (SG) (PDSI SG) whilst new governance arrangements are developed and put in place.
2.1 Living with a disability
There are 14.1 million disabled people in the UK.
- 8% of children are disabled
- 19% of working age adults are disabled
- 46% of pension age adults are disabled
Source: Family Resources Survey (2019 to 2020)
Graph 1 below shows disability prevalence by age group. 46% of disabled people are of state pension age, 19% of disabled people are working age adults, and 8% of disabled people are children. In total 22% of all people are disabled.
Graph 1. Disability Prevalence by age group
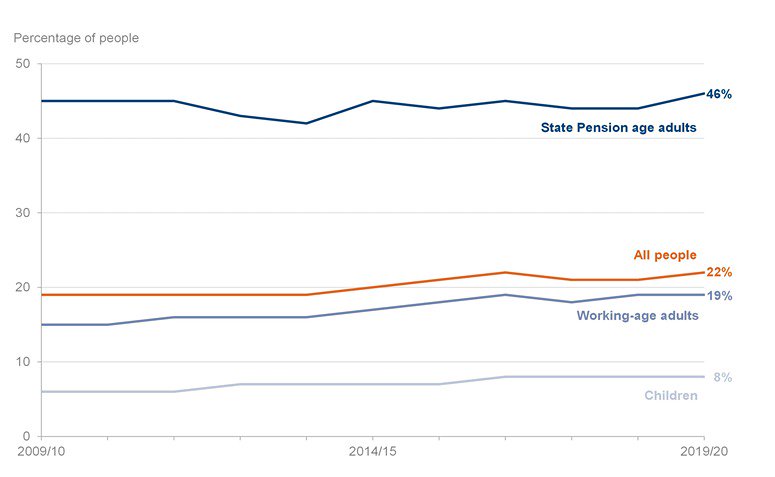
Source: Family Resource Survey 2019 to 2020 Disability
Graph 2. Disability Prevalence by age and gender
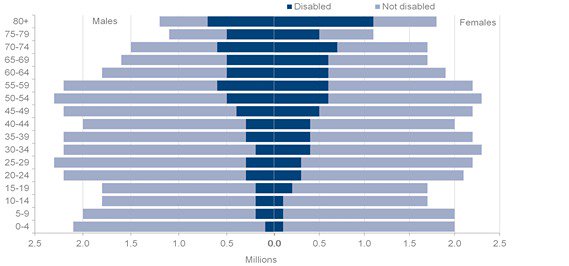
Source: Family Resource Survey 2019 to 2020 Disability
Graph 2 above shows disability prevalence by age and gender. There are more older aged females (65 years and above) living with a disability than males in the same age groups. Conversely, there are more male children aged 19 years and below living with a disability, than there are female children in the same age groups.
Graph 3. Impairment types reported by disabled people 2017 to 2018, 2018 to 2019, 2019 to 2020
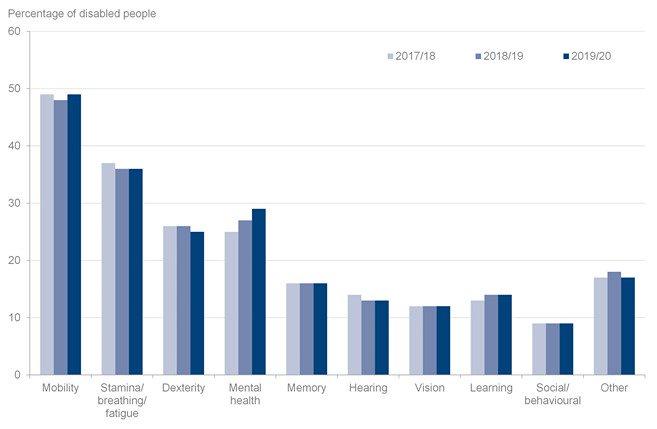
Source: Family Resource Survey 2019/20 Disability
Graph 3 above shows impairment types reported by disabled people between 2017/18, 2018/19 and 2019/20. The most frequently reported impairment type is mobility, with nearly 50% of disabled people reporting this impairment type.
2.2 Surrey context
Currently 3,300 individuals are known to Adult Social Care and have a Primary Client Category of Physical Disabilities recorded on LAS, Surrey County Council's case management system.
Table 1. below shows the breakdown of individuals known to Adult Social Care with a Primary Client Category of Physical Disabilities by age group.
| Ages Breakdown | Total | % |
|---|---|---|
| 18 to 24 | 173 | 5.20% |
| 25 to 34 | 210 | 6.40% |
| 35 to 49 | 606 | 18.40% |
| 50 to 64 | 1201 | 36.40% |
| 65+ | 1074 | 32.50% |
| Under 18 | 36 | 1.10% |
| Grand Total | 3,300 | 100% |
Source: Source: LAS snapshot August 2021
66.4% of people known to Adult Social Care with a primary client category of physical disability are younger age adults between 18 – 64 years old, and 32.5% are adults who are 65+ years old.
Young People with a primary category of physical disability in Surrey
170 young people between the age of 14 to 25 have a primary category of Physical Disability, of these there are 6 young people with Sensory Impairment as the Primary Support reason. Of the 170, 34 of these are under 18 years old (but, this figure is likely to be an under-representation as these are only the cases known to services at this current time).
Table 2. Number of predicted people to be requiring/receiving services 2010 to 2025 (18 years and older)
| Year | Total of clients | Community-based services in own home | Residential care | Nursing care |
|---|---|---|---|---|
| 2010 | 3,076 | 2,375 | 137 | 94 |
| 2011 | 3,093 | 2,387 | 138 | 94 |
| 2012 | 3,096 | 2,390 | 138 | 94 |
| 2015 | 3,126 | 2,413 | 139 | 95 |
| 2020 | 3,198 | 2,468 | 142 | 97 |
| 2025 | 3,261 | 2,517 | 145 | 99 |
Source: Adult Social Care Combined Activity Return (ASCCAR) and ONS population projections.
Table 2 shows the number of predicted people likely to require, or receive services, between 2010 and 2025 who are aged 18 years and older based on population projections for Surrey. There is likely to be a significant increased demand for community-based services delivered to people in their own home, and less demand for residential care or nursing care.
The current actual number of individuals (18 years and older) with a primary client category of physical disability known to Adult Social Care in 2021 is 3,300. This is slightly higher than the predicted numbers shown in Table 2. We need to further explore the reasons for this.
Where people live in Surrey
The table below shows the individual district and borough count of adults with physical disabilities living in each area. The highest number of adults with physical disabilities live in the Guildford and Waverly area.
Table 3: Client Category - Adults physical disability caseload by current address
| Borough or district | Number of adults with a physical disability |
|---|---|
| Waverley Borough Council | 459 |
| Reigate and Banstead Borough Council | 399 |
| Elmbridge Borough Council | 340 |
| Guildford Borough Council | 324 |
| Mole Valley District Council | 294 |
| Tandridge District Council | 269 |
| Woking Borough Council | 260 |
| Surrey Heath Borough Council | 254 |
| Epsom and Ewell Borough Council | 237 |
| Runnymede Borough Council | 231 |
| Spelthorne Borough Council | 231 |
Table 4. below shows the number of adults with a physical disability known to Adult Social Care who live within the county (3,289), and those who live out of the county (98) but still receive support from Adult Social Care services. Those people who are receiving support but do not live in the county are likely to be in receipt of services that are not available within Surrey.
Table 4. Current address summary for adults with a physical disability (updated 25 May 2021)
| Current address summary | Number of residents |
|---|---|
| In county | 3,298 |
| Out of county | 98 |
| Address not mappable | 11 |
| Address confidential | 69 |
Source: LAS Case list.
2.3 Living with sight loss
Over 2 million people in the UK are living with sight loss that has a significant impact on their daily lives. This figure includes people who are registered blind or partially sighted and those whose sight is just better than the level which qualifies for registration. It also includes people who are awaiting or having treatment and people whose vision could be improved by wearing correctly prescribed glasses.
Age is the key factor in the prevalence of sight loss. Areas that have a larger proportion of older people will have a higher estimated prevalence of sight loss when compared to an area with a younger age profile.
Sight for Surrey is commissioned by Adult Social Care to provide services to people with sight and/or hearing loss, and services to people who are Deaf. Sight for Surrey has approximately 5348 people with visual impairment on their database; this includes people who are registered as severely sight impaired/blind and sight impaired/partially sighted. Most of the users of this service are aged over 65.
The number of people of working age with a visual impairment is expected to remain stable to 2030, but with a 39% increase in prevalence in those over 65. The anticipated 39% increase (from 17,070 to 26,300 people) by 2,030 of people over 65 with a moderate or severe visual impairment is likely to challenge current service provision both in terms of volume and structure.
Not all people who use Sight for Surrey services will need to be eligible for Adult Social Care funded support. In addition to funded support, Sight for Surrey are able to offer access to information, advice, a helpline, small items of equipment, and specialist welfare benefits advice. Individuals can self-refer to these services.
2.4 Living with hearing loss
Estimates suggest 11 million people in the UK have hearing loss (source: hearinglink.org) – that's around 1 in 6 of the whole population. Levels of hearing loss – mild, moderate, severe or profound – are defined according to the quietest sound that you can hear. Hearing loss is an invisible disability making it easier for those living with hearing loss to be ignored or forgotten.
Sight for Surrey is commissioned by Adult Social Care to provide services to people with sight and/or hearing loss, and services to people who are Deaf. Sight for Surrey has approximately 1,398 people living with hearing loss on their database; this includes people who are Deaf and use BSL. Most users of this service are aged over 65.
The number of people of working age with a profound hearing impairment will remain stable over the next 2 years (at some 250 people), with a 15% rise (313 people) in those ages over 65 to 3667 people. This includes people who are Deaf and use BSL.
The numbers of adults with moderate or severe hearing impairment are much greater and the number will increase over the next 20 years at a higher rate.
In addition, Sight for Surrey also has approximately 1890 people living with combined sight and hearing loss on their database.
Not all people who use Sight for Surrey services will need to be eligible for Adult Social Care funded support. In addition to funded support, Sight for Surrey are able to offer access to information, advice, a helpline, small items of equipment, and specialist welfare benefits advice. Individuals can self-refer to these services.
2.5 Living with a long-term neurological condition (LTNC)
A long-term neurological condition (LTNC), sometimes referred to as a "neuro-disability", includes the range of conditions such as Acquired Brain Injury, Multiple Sclerosis, Parkinson's Disease and congenital and childhood conditions such as Cerebral Palsy, Muscular Dystrophy and Spina-Bifida and other rare conditions such as Motor Neurone Disease, Huntington's Disease and Progressive Supra-nuclear Palsy. (This is not an exhaustive list. Note Stroke for all ages is covered by the Older People's Strategy).
Long-term neurological conditions can be broadly categorised as follows:
- sudden onset conditions
- intermittent and unpredictable conditions
- progressive conditions.
- stable neurological conditions
According to the latest estimates, the total number of neurological cases in England has now reached 16.5 million, or an average of 75,000 cases per Clinical Commissioning Group (Source: Neuro Numbers 2019).
Although as a group LTNCs are relatively common, the number of people with individual conditions is rarely measured locally and it is difficult to obtain accurate data on specific conditions.
The time course of conditions also varies widely. The average time between diagnosis and death for someone with Motor Neurone Disease is 14 months, while someone with Multiple Sclerosis may live with the condition for decades. Even within specific conditions, the needs of individuals, for example for social care support, vary widely. A key feature of this strategy, therefore, is supporting people with long-term neurological conditions to live independently, often for many years.
2.6 Surrey County Council's expenditure on care and support (2020)
This section provides a snapshot of Surrey County Council's expenditure on care and support for 2020 to 2021.
Table 5. below shows the budget breakdown for physical disabilities and sensory impairment spend for 2020 to 2021.
| Adult Social Care Budget breakdown for Physical Disabilities and Sensory Impairment Spend | Full Year Budget | % of budget |
|---|---|---|
| Nursing | 5,966,569 | 13% |
| Residential General – External | 5,015,835 | 11% |
| Residential Dementia – External | 638,673 | 1% |
| Homecare | 10,171,528 | 22% |
| Supported Living | 2,411,879 | 5% |
| Extra Care Housing | 507,600 | 1% |
| Direct payments | 12,401,083 | 26% |
| Day Care – External | 688,655 | 1% |
| Respite Care | 309,896 | 1% |
| Transport Services | 72,052 | 0% |
| Other Care - External | 9,043,867 | 19% |
| Other Care In-House Provision | 0 | 0% |
| Total | 47,227,637 | 100% |
Table 5: PDSI budgets 2020/21 including contracts and grants and equipment
The largest amount of expenditure in 2020/21 for disabled people was on direct payments. Direct payments are a way for you to arrange your own adult social care support. Spend on direct payments represented 26% of the total expenditure for the 2020/21 financial year, with 904 individuals in receipt of a direct payment.
Table 5. below shows more up to date data on the active number of direct payment users between April 2021 and December 2021. The data in the table tells us in this period 631 people with a disability (29%) had an active direct payment, of which 395 people with a disability (63%) elected to use part of their direct payment to provide personal assistant support.
Table 6. Active direct payment client numbers April to December 2021
| April – December 2021 - Active Direct Payment clients | Older People | Physical Disability | Mental Health | Learning Disability and Autism | Transition | Carers | Total |
|---|---|---|---|---|---|---|---|
| Number of direct payment users | 523 | 631 | 63 | 533 | 243 | 196 | 2189 |
| Of which this number have a personal assistant | 171 | 395 | 12 | 281 | 173 | 2 | 1034 |
| Use of a personal assistant as a % of total direct payments | 33% | 63% | 19% | 53% | 71% | 1% | 47% |
Source: Adults' Social Care System (LAS). Table 6. Active direct payment client numbers April – December 2021
Of the 631 people with a disability receiving a direct payment between April – December 2021, 551 were aged between 18 – 64 years old, and 80 were 65 years old or older.
Homebased care is the next largest reason for expenditure, at 22% of the budget (for 767 individuals), and other care purchased from external community providers at 19%. External community providers include the district and borough councils who provide Handy Person and Home Improvement services; the countywide Community Equipment Service; spend on Blue Badges; spend on information and advice service and welfare benefits advice; spend on day opportunities; peer support through Surrey Independent Living Council (SILC); user engagement through Surrey Coalition of Disabled people; and the Combined Sensory Services contract delivered by Sight for Surrey. There are initiatives underway to improve access for people with disabilities to these initiatives. For example, the specification for Handy Person schemes (which is available to younger adults (18 years+) with disabilities), funded by the Better Care Fund, is being refreshed and the outcomes expected from the schemes will be made clearer.
It should also be noted that 5% of expenditure related to supported living provision (for 125 individuals). Reassuringly, this shows that 72% of total expenditure was spent on care and support in community-based provision and settings aimed at sustaining and maintaining disabled people's independence and autonomy in their own homes. The Accommodation with Care and Support strategy aims to increase the availability of accessible supported independent living accommodation options for people who are disabled. For people living in their own homes who might require structural changes to make their home more accessible the Disabled Facilities Grant (administered by the district and borough councils) is available to help make these changes.
Although 25% of expenditure related to residential and nursing care, we know that within this percentage there will be a sizable number of people who entered these services primarily because of needs related to ageing, rather than solely related to their disability. The need for specialist dementia care is a good example of this. As people with disabilities age and may enter a residential care setting we will need to ensure such settings have a workforce who are suitably skilled and trained, alongside models of service delivery that might need to be more tailored and personalised to take account of disabled people's needs.
Section 3. Promoting positive health, wellbeing, resilience, and independence
Contents
- 3.1 Barriers to achieving positive health, wellbeing, resilience, and independence in Surrey
- 3.2 Disabled people's personal wellbeing during the coronavirus pandemic
- 3.3 Community and financial inclusion
- 3.4 Financial inclusion
- 3.5 Advocacy
- 3.6 Signposting
- 3.7 Health and social care services
- 3.8 Technology
- 3.9 Staying active
- 3.10 Employment
- 3.11 Housing
The Care Act 2014 gave new statutory duties to local authorities to support people to maintain their wellbeing and independence. The act enshrines the principle of individual wellbeing, placing this at the heart of the care and support system. It promotes independence and cites the importance of partnership working, with a drive towards greater integration between different services to improve people's outcomes.
An individual's or community's wellbeing depends on many issues, including:
- people's interest and engagement in the community, and their sense of control over their own lives
- happiness and feelings of confidence and self-esteem
- being treated with dignity and respect
- access to affordable, nutritious food
- a sense of security – financial and otherwise
- access to services, facilities and opportunities
- the care and support that is available when needed
- comfort and overall quality of life
- spiritual needs and respect for faith and religion
- access to affordable, safe, secure and appropriate housing
- protection from crime and disorder
- people's work, home and recreational environments
So, it is important to acknowledge how the negative attitudes of others have significant impacts across all areas of disabled people's wellbeing and help to create the barriers disabled people face. Feedback from Surrey Coalition and the user forums and groups tells us there are wide-ranging impacts of negative perceptions on disabled people, for example loneliness, barriers to employment, or the worry of being insulted or harassed. Actions which (even unintentionally) isolate or exclude disabled people can cause significant adverse impact on positive health, wellbeing, resilience, and independence.
Action at a local level is essential to create inclusive and enabling communities and it is vital that local authorities, local health bodies, NHS trusts, the third sector, businesses and other service providers work co-productively with disabled people and representative organisations led by disabled people to identify problems and solutions and make the most of opportunities to improve services.
We would expect:
- all disabled people will need access to good quality, accessible information, advice and universal services to help Prevent need
- many disabled people would benefit from early help or targeted support to Reduce need later in life
- some disabled people will need help and support quickly. Doing this well can Delay increased need
- fewer people will have a need for ongoing support to Meet their needs
3.1 Barriers to achieving positive health, wellbeing, resilience, and independence in Surrey
The barriers identified by disabled people in Surrey reflect the concerns identified nationally; including barriers in accessing information provision, transport, housing, the physical and built environment, access to healthcare and personal assistance. People told us they also faced additional barriers in relation to low income, social attitudes to disability, and psychological barriers such as low self-esteem.
The list below summarises the key concerns of disabled people in Surrey and the need for action and improvement in the following areas:
- accessible community facilities, including leisure, and accessible outdoor resources
- involvement in worthwhile activities (through work and life-long learning), and opportunities to increase social participation
- more focussed personal care and support that enhances dignity
- more consistent and timely access to physical and psychological rehabilitation services that continue through community-based services on discharge from hospital
- increased provision of therapy services, including access to NHS counselling services, across the whole health and social care system
- improving access to technology enabled choice and control
- improving access to adapted social housing for working age adults
- improving access to disability benefits advice
- integration of health and social care where this makes the most sense to do so
- staff are appropriately skilled and trained to work with disabled people, and are supported to maintain competence in their roles
- identifying the areas of corporate responsibility – housing, public places, general access, attitudes, culture, and thinking about the bigger picture
- acknowledging the impact of Covid specifically on disabled people
These were recognised as inter-connected. Efforts to enhance wellbeing must harness contributions from across the full range of Surrey County Council functions, including adult social care, public health, community safety, health promotion, environmental improvement; alongside the NHS; and Surrey's district and borough council functions related to housing, transport, and leisure. Each contribution being part of a jigsaw needed to be complete to create a truly enabling Surrey. Tackling these challenges requires real partnership working. In particular, we know we will only make more progress and achieve better results if we work with disabled people, so that we understand the issues properly and find solutions that work.
We will: Establish a new governance structure, co-produced with disabled people, to ensure disabled people are part of discussions about how plans for actions creating better opportunities and outcomes are developed and reviewed.
We will: Ensure the policies and practices of partner organisations provide equality of access and opportunity.
We will: Ensure disabled people are fully involved in identifying their needs, designing services and solutions to address these and in being part of the response.
Analysing the feedback from the Surrey user forums showed some areas of concern were consistently mentioned as areas requiring greater investment, greater improvement, or were considered to have greater importance if we are to support people to reach their full potential. These are set out below.
3.2 Disabled people's personal wellbeing during the coronavirus pandemic
All the Surrey user forum's reported concerns about their own, or other disabled peoples' wellbeing during the coronavirus pandemic. Some people felt there had been a further erosion of disabled people's rights; others reported increased levels of mental distress because of loneliness, increased anxiety, and the discriminatory or marginalising treatment of disabled people. Essentially the pandemic shone a light on the pre-existing inequalities and barriers disabled people face, and how the effects of the pandemic have been felt more acutely by disabled people, with implications for digital inclusion, work, and access to support and care at home. In February 2021 the Office for National Statistics published data describing the effect coronavirus had on disabled people. This is shown below.
Coronavirus and its effect on disabled people, in February 2021, around two-thirds (65%) of disabled people reported the coronavirus (COVID-19) affected their wellbeing compared with half (50%) of non-disabled people.
Disabled people more frequently than non-disabled people indicated that the coronavirus was affecting their wellbeing because:
- it makes their mental health worse (46% for disabled people and 29% for non-disabled people)
- they are feeling like a burden on others (25% and 10%)
- they are feeling stressed and anxious (67% and 54%)
- they are feeling lonely (49% and 37%)
- they spend too much time alone (42% and 31%)
- they have no one to talk to about their worries (24% and 16%)
Source: Coronavirus and the social impacts on disabled people in Great Britain: February 2021 (Office for National Statistics)
Coronavirus further exacerbated the barriers already faced by disabled people in daily life which made them more chronically lonely than non-disabled people. For example, some people never stopped shielding or isolating even when pandemic restrictions eased. We know the degree to which individuals are interconnected and embedded in communities has a powerful impact on their health and wellbeing.
This strategy gives us the opportunity to look back at the lessons learned from the pandemic – for example, everybody is not treated equally, especially in a pandemic – and use these lessons as a driver for real change in breaking down the barriers to inclusion. Yet in the pandemic there have been some positive developments for people with disabilities. Where they can get internet access, people with disabilities have been able to participate in society as never before, because physical and communication barriers have largely disappeared as education, work, shopping, and many leisure activities have been driven online. People with disabilities do not want a return to the pre-pandemic status quo. A better future must grow from learning the lessons, listening to the life experiences of people with disabilities, and taking meaningful actions that improve the health, wellbeing, resilience, and independence of people with disabilities.
Loneliness: Loneliness data is collected the Community Life Survey (CLS) covering England for the year ending March 2019. Definitions for loneliness can be found in the accompanying methodology article's glossary.
The data shows a significantly higher percentage of disabled people aged 16 years and over felt lonely compared with non-disabled people. The proportion of disabled people (13.9%) who reported feeling lonely "often or always" was nearly 4 times that of non-disabled people (3.8%).
The largest disparity between disabled and non-disabled people was seen for the 35 to 49 year age group (17.8 percentage points). While the level of loneliness for disabled people was among one of the highest (20.6 %) in this age group, the level of loneliness for non-disabled people (2.8%) was significantly lower than younger non-disabled people. Source: Community Life Survey March 2019
3.3 Community and financial inclusion
"The pavements are in such a state that for anyone who is blind or partially sighted, or those with a mobility impairment, freedom of movement is non-existent". (User participant, DENS, 2021)
Community inclusion is the experience of visiting, belonging, sharing and using the facilities available in the ordinary places that define the local community life where people live. It means the extent to which individuals participate in a variety of valued activities, including leisure and work. It is also the experience of being part of a growing network of personal relationships and the valued contribution which may be made by the individual to these relationships, and to activities that are part of their local community. Many disabled people rely on publicly funded services to make this happen.
Consultation feedback – community inclusion
- supporting and promoting the independence of disabled people is not just a health and social care responsibility but one for the whole community
- more needs to be done by 'Corporate Surrey' to change public attitudes towards disability from one where disabled people are defined by their impairment, to one where there is an acceptance that society needs to make adjustments so that disabled people are able to take up the same opportunities and make the same choices as everyone else
- supporting people who are disabled to lead independent lives is not just a health and social services responsibility but the responsibility of the wider system (for example transport, housing and so on) to improve social inclusion
- lack of accessible mainstream transport which people can safely use (only available on some routes and at certain times and particularly poor in rural areas)
- lack of specialist transport / escorts when these may be required, especially if needed at short notice
- poor transport information which is hard to access and poor staff awareness of disability issues
- identify the areas of corporate responsibility – housing, public places, general access, attitudes, culture, and think about the bigger picture – and work to improve these together
The Let's Hear Group, part of Surrey Coalition of Disabled People, is a proactive group of hearing aid users who visit towns across Surrey to assess the hearing loop provision in shops, cafes and other businesses. The aim of the group is to raise awareness, educate and advise. The group have already succeeded in raising awareness of hearing loops to a national fashion retailer who have since rolled out training in their stores across the country.
Access groups are supported by district and borough councils and are aimed at people with any particular access needs, including those with a sensory, physical or cognitive disability. The local access groups highlight access barriers at a community level – for example, inaccessible design, access refusal (for assistance dogs), transport barriers, as well as getting involved in more proactive work with planning departments within borough and districts and some local influencing on issues such as the installation of changing places toilets. There is a geographical variation in the provision of access groups in the county – with some borough and districts no longer supporting a group, some groups no longer being active and others having quite strict criteria as to who can be involved. There is also not a countywide access group – particularly relevant for people who live in one part of the county but work in another, where the access barrier may well be in their work area. In order to make strategic progress on removing access barriers for disabled people, we need to reduce the variation in the provision of these groups as well as introducing a countywide access forum. Access groups could support planning committees and this should be developed as part of the process.
Surrey County Council are in the initial stages of undertaking a prevention spend mapping exercise to gain a clearer initial picture of SCC's prevention spend and activity, from which specific opportunities and areas of work can be identified. It will also support SCC to start looking at prevention in a more cross cutting way across our teams and functions, thinking about spend, activity and impact for communities and places. It is proposed that the approach to Prevention Spend Mapping aligns with the Health and Wellbeing Strategy framework of Start Well, Live Well, Age Well, with consideration of priorities and inequality.
Community connections services are key part of the mental health early help offer for adults in Surrey. The services are delivered by 3 voluntary sector lead providers (Catalyst, Mary Frances Trust and Richmond Fellowship). They are universal access services that support people with mental health needs to stay well in their communities through social connections and networks. Throughout the pandemic, Community Connections services have substantially grown their online virtual offer. Groups include regular drop-in sessions as well as a substantial training offer, arts and crafts, photography, and self-help/peer support groups for a range of different needs and are inclusive of people with physical and sensory impairments.
We will: Develop on the work currently underway to pilot initiatives to support communities and neighbourhood to be genuinely accessible and thereby welcoming to autistic residents is developed to address barriers to community inclusion for other population group.
3.4 Financial inclusion
There is a strong correlation between disability, poverty and financial exclusion. The story of disabled people's financial inclusion is a complex one and is not simply linked to a lack of money. Research by Scope shows that 1 in 8 (12%) disabled people cannot physically access their bank; 1 in 12 (8%) want to protect themselves against financial crises but feel they are turned down for insurance. More than one-fifth (22%) said they are forced to pay higher premiums because they are disabled. Scope also found that a majority of websites and apps do not meet suggested UK government guidelines on accessibility. This makes it harder for people who are visually or hearing impaired or experience cognitive issues to find the products and services they need at affordable prices.
Consultation feedback – financial inclusion
- how do we improve access to disability benefits advice? For example, improving signposting to benefits advice and services at an earlier stage?
- how do we improve employment support so that more people can start and stay in work?
- how can Surrey County Council as an employer better support disabled people and those with long-term conditions if they are in work?
We will: Review the current accessibility of specialist benefits advice in Surrey as part of the broader piece of work increasing access to benefits advice to all residents.
We will: As part of the work to look at the employment support that is available, we will review the support available to employers to make reasonable adjustments and offer equitable access to work opportunities.
We will: Review SCC's own employment policies to ensure that people with disabilities have equitable access to employment.
We will: Ensure sufficient use is made of internships and apprenticeships to support people with disabilities seeking to develop their work experience and skills
3.5 Advocacy
Advocacy is taking action to help people say what they want, secure their rights, represent their interests, and obtain services they need. Advocates and advocacy schemes work in partnership with the people they support and take their side. Advocacy promotes social inclusion, equality, and social justice.
Care Act Advocacy is jointly commissioned in Surrey for all people going through any stage of a care assessment, support plan and/or review including safeguarding processes.
Consultation feedback - advocacy
- not all disabled people will need Care Act Advocacy but do want to influence policy, and decisions, and to change the "what is" into a "what should be"
- access to general (non-specialist) advocacy is an area that is underdeveloped
We will: Continue to deliver inclusive statutory and non-statutory advocacy services for Surrey residents including promoting this offer more widely
3.6 Signposting
Signposting is directing people to other individuals, charities or third parties who can help them. Effective signposting is dependent on a good understanding of other local and national organisations.
Consultation feedback - signposting
- more focus on front line staff developing a working knowledge and confidence in how other services operate, what they have to offer and how to refer to them
- publicising Surrey Coalition and other 'sources of support' organisations to front line staff
We will: Work with colleagues from corporate communications and the adult social care information and advice team to ensure disabled people have the information, advice and guidance required to make good informed decisions about their care and support, and have ready access to up-to-date information and advice about rights and services
We will: Develop a web based physical disability and sensory impairment information/resource hub
3.7 Health and social care services
"We all need help, but if you have a significant physical disability this means that you will need ongoing and regular help". (User participant, DENS, 2021)
People with disabilities report facing structural, financial, and cultural/attitudinal barriers when they seek to access health or social care. Difficulties in accessing health and social care can be caused by lack of transport, inaccessible buildings, and inadequate training of health and social care professionals, among other factors. People with disabilities say that they feel their needs are not understood, that they do not feel listened to and that they are perceived as low priority due to their pre-existing condition. These problems have all been exacerbated by Coronavirus (Source: Consultation Feedback, 2021). Where people were in receipt of services 48% reported they had enough choice about their care and support services. (Source: Physical and Sensory Disability Survey, SCC, 2021).
The consultation feedback felt it important to recognise younger disabled adults' access social care for different reasons, and their desired outcomes may vary significantly. Younger disabled adults often need help but can be seen as too independent for support. Research shows that younger disabled adults who seek social care support are more likely to end up with no services received or being signposted elsewhere, compared to older adults (65 years+) seeking support. The consultation feedback stressed that younger disabled adults rely on social care to lead independent, healthy lives, and when done right, it empowers them not just to live, but to have a life.
Consultation feedback – health and social services
- more focussed personal care and support that enhances dignity and choice
- acknowledge the reasons younger disabled adults' access social care are different than for older adults, tailor and personalise the experience of services
- provide more consistent and timely access to physical and psychological rehabilitation services that continue through community-based NHS services on discharge from hospital
- periods of rehabilitation should be longer and rehabilitation teams need to be integrated across services. People felt that the current focus of rehab was short and did not respond to the changing and long-term needs of disabled people
- increased the provision of therapy services, including access to NHS Counselling services, across the whole health and social care system
- integrate health and social care where this makes the most sense to do so
- acknowledge the impact of Covid specifically on disabled people
- assessments by health and social care do capture the multiple conditions/needs an individual might have, so all the needs of that person may not be clear
- assessments should include reference to the social context for that person
We will: Collaborate and co-produce services with the community and voluntary sector who are often closer to residents and already meeting health and social care needs for some of individuals
We will: Work closely with NHS operational teams to improve care pathways and achieve better health outcomes for residents
We will: Work closely with the Communities and Prevention team, local systems, health and the community and voluntary sector, to promote better community support services and opportunities to remain healthy, well and active for longer
Consultation feedback – health and social care workforce
- access-4-ALL designs to be embedded in the working practices of all staff planning and delivering services. If disabled people have to challenge the provider because any feature is inaccessible due to poor policies or practices, then the design is flawed
- Adult Social Care staff should be given training to understand that people are experts in their own condition
- more staff at all levels should have their skills and understanding refreshed frequently by contact with users and carers life experience from outside their area of service delivery
- more staff with lived experience of disabilities should be recruited to inform and improve the skill set of existing staff
- workforce training on different conditions, and the impact of different conditions
- as a minimum make sure all people are connected to sources of information, advice, and advocacy
- speed of response/prioritising especially for certain conditions that can progress quickly
- emergency signposting needs to be available as people approach end of life
- all members of the group felt they did not have enough choice about their care and support services and that there should be a way to contact Adult Social Care for advice. The system is very complicated and there is no way that someone with additional needs could access support on their own. The system can be a challenge and needs to be more accessible for the service user rather than having to rely on a carer to help them access it
- not easy to find this assistance even if you are able to pay or contribute to this
The ever-changing nature of adult social care means providing personalised, preventative, and quality care and support services is a challenging process. Our overall aim for our workforce is to have the right workforce doing the right things at an achievable cost. This means raising workforce professionalism, capacity, competence, and standards to enable user choice, control and autonomy; and improving partnerships with health, housing, leisure, sport and employment.
We will: Continue to invest in practice improvement and continuing professional development of adult social care practitioners.
We will: Improve ways of working within adult social care, with a focus on improvement ensuring we continually develop to reflect changes in best practice, national and local policy, and operational issues.
We will: Get better at sharing expertise and knowledge across staff and teams, and create opportunities for refreshing understanding and skills in relation to the lived experience of disabled people.
We will: Ensure information and advice is easily available and accessible.
We will: Review our information and advice content to ensure there is reference to emergency signposting as people approach end of life.
3.8 Technology
"Technology helps me to do what I want to in life, but it can be difficult to keep up with my non-disabled peers because there is a lack of knowledge around tech, and it is less affordable for people who are on low incomes". (User participant DENS, 2021)
Technology offers a range of potential solutions to many of the everyday challenges that disabled people face. This can be most convenient and accessible when integrated in products designed for all, such as smartphones. Other assistive products are more specialised, such as wheelchairs, hearing aids or screen readers. The impact of products that support everyday tasks is huge.
Too often technology is developed without taking account of the needs of disabled consumers. From streaming services and smartphone apps to artificial intelligence-powered recruitment and interview tools, the importance of involving disabled consumers in the design process is crucial.
The COVID-19 pandemic has increased the importance of assistive and accessible technology for many disabled people and reminded us that access to the right technology is key to unlocking greater inclusion. Digital exclusion matters because it is linked to loneliness and isolation and the wider determinants of health (including poverty, income, and employment). In addition, digital inclusion is essential in laying a solid foundation for the future use of Technology Enabled Care, which many disabled people may be able to utilise.
Consultation feedback - technology
- improving access to technology enables choice and control
- equality of access to the internet/connectivity is important
- technology can act as an enabler for early intervention and prevention
- organisations should share online resources
We will: Seek to innovate and make best use of technical solutions to address gaps in provision making sure the needs of all people including people physical disabilities and their carers' are always considered
We will: Make the most of assistive technology to support a person centred approach to care and support, enabling the individual to remain in control and independent
We will: Invest in digital inclusion initiatives to ensure access to information and advice, and support and care, can be achieved virtually
The Tech to Community Connect project is a collaborative effort between Surrey Coalition, Action for Carers Surrey, Surrey Minority Ethnic Forum and many other partners. It provides technology (for example, tablets, smartphones and smart speakers), support in using technology and virtual groups to reduce feelings of loneliness and isolation in people with care and support needs across Surrey. A team of volunteers called 'Tech Angels' support participants to help them learn how to use the technology, give some training in how to stay safe online and offers a selection of 'modules' to choose from, including shopping online, online banking, accessing green spaces, booking and attending virtual health appointments, staying active online, listening to music, joining groups and many more.
The Enabling You with Technology Programme is to design and deliver a technology-enabled care offer, with the aim of supporting people to live independently in their own homes for as long as possible. Technology-enabled care can enhance the care and support provided by carers and others, right-size the care package required and, in some cases, replace reduce the need for personal care, thereby increasing independence. The programme is in the early design phase, testing technology and approaches prior to rolling out a service countywide.
3.9 Staying active
"I want to know that I am welcome in non-disabled sessions. Sometimes you only see disabled people on posters for disabled sports". (User participant, DENS, 2021)
The Physical Activity Strategy 'Movement for Change' is a high level plan that supports Surrey's Health and Wellbeing strategy. It encourages a new way of working to help everyone adopt a more active lifestyle, with a particular focus on those who need it most.
There are lots of activities that are inclusive of disabled people in Surrey but knowing where to find them can be tricky. Use the Get Active Activity Finder to find out what activities are available.
Consultation feedback – staying active
- accessible community facilities, including leisure, and accessible outdoor resources
- some Surrey County Council and district and borough buildings are not accessible
- the lack of accessible or available transport can hinder or prevent disabled people from staying active
We will: Support Active Surrey and the 'Movement for Change' strategy to ensure mainstream leisure and outdoor resources continue to welcome disabled people, and help them achieve a more active lifestyle.
We will: Promote opportunities for inclusive activities in Adult Social Care advice and information material, and ensure disabled people know where to find this.
We will: Work with social prescribing and green prescribing services to ensure these services are accessed by all surrey residents who could benefit from them.
We will: Use our strategic review of transport and travel in Surrey to ensure that the needs of Disabled People inform planning for the future.
We will: Through our Community Inclusion workstream in Adult Social Care Commissioning, explore the barriers to community inclusion that disabled people experience and develop with stakeholders action plans to address them.
Wheels for All encourages all children and adults with disabilities and differing needs to engage in a quality cycling activity. Using specially adapted cycles, the activities are both physically and mentally stimulating and above all fun. All the centres are equipped with specially adapted cycles and Wheels for All trained leaders, who have the knowledge and confidence to work with participants so they can enjoy the benefits of cycling. The centres welcome individuals, groups and families and in Surrey are located in Epsom, Leatherhead and Woking. Find out more on the Wheels for All website.
The new Eastwood Leisure Centre at Sheerwater represents a £26m investment by the council into improving the health and wellbeing of residents in Sheerwater. This is the borough's most inclusive sports facility to date with 2 Changing Places changing rooms; a pool with moveable floor, hoist and privacy blinds; and changing rooms that can be partitioned for different groups and activities.
3.10 Employment
"I have found it hard to get a job. Partly, because there does not seem to be any help, and also because employers do not seem to understand disability and are a bit frightened of it". (User participant, DENS, 2021)
The Office for National Statistics (ONS) publishes quarterly updates on the labour market status of disabled people.
These can be found in the Labour market status of disabled people datasets. Based on the Labour Force Survey (LFS), these tables showed that around half of disabled people (52.1%) aged 16 to 64 years in the UK were employed in 2020 (July to September 2020) compared with around 8 in 10 (81.3%) of non-disabled people.
Graph 4. Below shows the employment rates of people aged 16 to 64 years captured over a 6 month period January to June 2020.
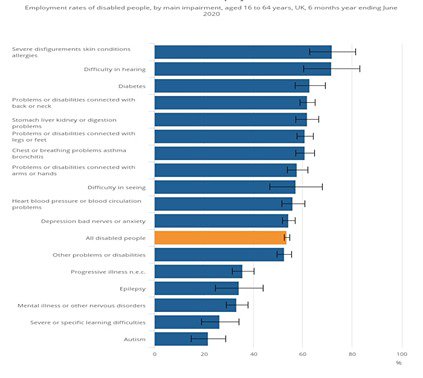
Source – Office for National Statistics
Consultation feedback - employment
- more needs to be done to understand what is on offer relating to employment for people who are disabled
- more needs to be done to understand younger disabled adults' perspective on employment, access to vocational programmes, and experience of being in employment
We will: For those able and ready to work, we will work with existing employment initiatives and employment support services to ensure better connections with Adult Social Care as an active partner in developing employment pathways for people with disabilities
We will: As a council use our own resources to develop and sustain employment pathways for people with disabilities through apprenticeships, making reasonable adjustments, and challenging negative attitudes
We will: Develop a performance indicator to capture employment rates of disabled people in Surrey and use this to work on improving access to employment opportunities
The Hidden Talent Programme, developed by the council's Communities and Prevention Team have been working to support employment opportunities for people with disabilities and additional support needs, so that hidden talent is released to help Surrey businesses thrive Between June – July 2021, 151 residents were contacted or engaged (99 over Zoom, and 52 via Surrey Says survey) from the target group (those 18+ with additional needs and disabilities) to understand barriers to accessing jobs what employment support would be helpful, and how businesses can make the workplace more accessible. SCC are currently drafting a report to summarise the findings from the user engagement, showing that for those engaged with the most common barrier to employment are perceived as the employers' mindset including:
- negative attitudes of business towards hiring those with additional needs and disabilities
- lack of awareness from businesses of the types of reasonable adjustments they can offer and Access to Work
- lack of awareness from businesses of the benefits of hiring those with additional needs and disabilities
As part of the 'No one left behind programme', Surrey County Council has undertaken a piece of work with Surrey Coalition to begin to map vocational programmes across Surrey and to bring providers of vocational programmes for disabled people together, to work together on improving access to the programmes and developing a greater level of knowledge about what is on offer.
3.11 Housing
"Advice and help with housing and benefits is really important. It can feel very isolating". (User participant, DENS, 2021)
Nearly 1 in 4 (24.9%) of disabled people aged 16 to 64 years live in rented social housing compared with less than 1 in 10 (7.8%) of non-disabled people, a significant difference. Disabled people were significantly less likely to own their own home (40.9%) or to live with parents (15.6%) than non-disabled people (53.4% and 18.6% respectively).
The housing situation of disabled people varies across age groups. Young disabled people aged 16 to 24 years were as likely to live with parents as non-disabled people of the same age, with similar proportions seen for each (71.7 % for disabled people, 74.4% for non-disabled people). Disabled people in older age groups, up to age 49 years were significantly more likely to live with parents, with the largest disparity seen for ages 30 to 34 years, at which age 15.5% of disabled people lived with parents compared with 9.5% of non-disabled people. (Source: Office for National Statistics, June 2020)
The supply of private and social rented housing suitable for disabled people is very limited in Surrey. There is an acute shortage of social rented housing and many applicants on the (11) district and borough council housing registers have long waits for rehousing.
Consultation feedback - housing
- affordable, suitably designed and accessible homes in the right places, with supporting infrastructure, can extend independent and safe living for older people and working age disabled people and/or other long-term health needs
- more training for Occupational Therapists on different conditions
- more involvement from Occupational Therapist in the initial development and design of accommodation for people with disabilities
We will: Ensure the new Surrey Adult Social Care Accommodation with Care and Support Strategy specifically addresses the availability and accessibility of new housing options for disabled people across Surrey
We will: Work with the council's property team, the district and borough councils, the private sector and independent sector, to identify development opportunities for new build accommodation in Surrey
We will: Work with housing colleagues from the sectors above to identify current housing stock and consider how this might be redesigned to create more suitable and accessible homes
We will: Where appropriate work with the borough and district housing teams to improve the information and advice regarding local housing options available to residents of their area, and how to access them
Surrey Adult Social Care Accommodation with Care and Support Strategy
Working together with our colleagues in the council's property team, providers, the NHS and the district and borough councils to supported independent accommodation for over 500 people will be developed over the next 5 years:
- building new accommodation
- developing existing accommodation
- changing the way care is provided to support greater independence and community inclusion
Section 4. Services to Support Independent Lives
4.1 Current supply of services for people with disabilities (including LTNCs)
Adult Social Care commissions and provides a significant amount of care and support for people with disabilities, people with sensory impairments, and people with a long-term neurological condition (LTNC's). This includes help at home, day opportunities, and residential/nursing spot placements; complemented by a range of NHS provided support (including funded rehabilitation). Many of the services accessed by people with disabilities are also generic universal services, but there can be barriers such as structural issues related to physical access into buildings, or a lack of transport for example, preventing equal access.
Specific services for people who are disabled (including LTNCs)
The below list sets out the specific services for people who are disabled (including people living with LTNCs) across Surrey. Also included are the generic services like Millbrook, who provide generic services to all residents in Surrey.
Contracts (block)
- Sight for Surrey
- Stroke Association
- small amounts across Better Care Fund across various voluntary sectors
Day Opportunities
- Headway (acquired brain injury)
- White Lodge
- Disability Initiative
- Bletchingley Skills Centre
- Surrey Choices
- Employability
Top Supported Living
- Seeability
- Royal National Institute of Blind People (RNIB) - Charity
- Wellmede Housing Association
- Active Prospects
- Achieve Together
Top Residential and Nursing
- Queen Elizabeth Foundation
- (Neuro rehabilitation)
- Leonard Cheshire (Hydon Hill)
- The Meath
- The Woodlarks Centre
- The Disabilities Trust
User Engagement (Physical disability or sensory impairment specific)
- Surrey Coalition (including Surrey Coalition Newsletter)
- Hard of Hearing forum (includes Surrey Deaf Community)
- Surrey Vision Action Group
- Long-Term Neuro Conditions Group
Other (Generic services)
- Equipment: Millbrook and Queen Elizabeth Foundation
- Home Based Care
- Specialist Health Professionals (for example Parkinson's Nurses)
- Home Improvement and Handy Persons
- Blue Badge Services
- Other Residential and Nursing
Daytime support (including aspects of community rehabilitation support):
- Headway Surrey
- Disability Initiative
- White Lodge
- Bletchingley Skills Centre
- Surrey Choices (Frenches Lodge, Woking Resource Centre, Nexus)
Equipment Support:
- Millbrook Healthcare
- Queen Elizabeth Foundation
Residential Rehabilitation Support (commissioned on a spot order basis):
- Queen Elizabeth Foundation
Blue Badge services:
- Various providers
Home Improvement Agency and Handy Person Schemes (through Surrey district and borough councils)
- Various providers
Employment support:
- Employability
Health commissioned support
- primary care is commonly the presentation and referral point into services although for some people this may be via secondary care through presentation to Accident and Emergency.
It is likely, therefore, that the person with a physical disability will require a range of agencies and services over time, to support their independence including health and social care, voluntary and independent sector resources, as well as services such as transport, housing, employment, education, benefits and pensions.
Most of the care for people with neurological conditions takes place in outpatient neurology clinics or in the community. Yet with existing datasets it is not possible to know what condition an individual attending a neurology appointment has, nor whether the appointment was relating to diagnosis or ongoing management of a condition.
Current supply of services for people who have a sight and/or hearing loss, or who are Deaf
Sight for Surrey is commissioned by Adult Social Care to provide services to people with sight and/or hearing loss, and services to people who are Deaf. Services include:
- information, advice and assessment
- communication support, and BSL sign language interpreting services
- equipment for the home and for accessing the community
- support to obtain a Certification of Vision Impairment (CVI)
- assessment and rehabilitation support
- Eye Care Liaison Officers (in hospitals)
- specialist social work support (including assessment and safeguarding)
- specialist welfare benefits support
Surrey Heartlands Clinical Commissioning Group commissions a wide range of eye care services. Eye care services cover all services designed to enable people to maintain good eye health and sight, or to maintain and make best use of remaining sight when sight loss that cannot be corrected has occurred. Eye care services are provided by a wide range of providers and professionals including GPs, ophthalmologists, hospital and community optometrists, dispensing opticians, health visitors and voluntary sector providers.
NHS Audiology services are provided in hospital and primary care settings, and through the independent sector, across Surrey.
Direct payments
Surrey County Council is working in partnership with Surrey Coalition of Disabled People and We Coproduce to create a new strategy for direct payments across the whole of Surrey. A direct payments survey has been circulated to gain feedback on people's experience of direct payments, how they are working now, and how they can work better. The survey closed on 10 January 2022. The feedback from the survey will be used to inform the new Surrey wide strategy for direct payments.
We will: Do more to ensure that residents are able to use their direct payment in a way which maximizes their independence
We will: Use the results of the direct payments survey to refresh our direct payments offer to Surrey residents
Co-producing the Market Position Statement
We will co-produce a market position statement that sits alongside this strategy and the strategy action plan.
A market position statement sets out a local authority's ambitions for working with providers to encourage the development of a diverse range of care and support options. It can include statements about local demand for different care and support options, the local authority's vision for care and support, and commissioning policies and practices.
We will prioritise the following areas to support Surrey County Council's 3 corporate strategy goals of wellbeing, economic prosperity and resident experience:
Information and advice – Providing information and advice to residents to promote their independence, health, and wellbeing.
Technology and innovation – Using technology to promote independence, health, and wellbeing, and manage increasing demand by driving proportionate practice. We will seek out opportunities, and maintain an awareness of technology innovation and trails, that help to upskill our workforce, learning from others what works well.
Community based support and direct payments –Working collaboratively with partners and providers in the community making best use of direct payments, existing community assets, and services.
Carers – Supporting individuals that provide unpaid care and support to family and/or friends to enable them to continue their caring role.
Home based care –Working with providers to deliver care and support to individuals in their own home to promote their independence and delay the need for accommodation-based care.
Market management –Working collaboratively with partners and providers to deliver high quality services and affordable and sustainable prices.
Accommodation with care and support – Developing a range of flexible and financially sustainable accommodation with care and support that will enable adults to live and age well in Surrey.
Section 5. Supporting carers and families
A carer is someone who provides unpaid help and support to a family member, partner, friend or neighbour. Carers include adults, parents or children and young people. They might be adults looking after other adults, parent carers looking after children with a disability, and young carers under 18 years of age. Carers may provide emotional as well as physical support. Without the care they give, those benefiting from their help would find difficulty managing or may be unable to cope, yet on average for 25% of carers it takes 5 years to recognise themselves as a carer.
There is no typical carer, as each carer's situation is unique to them. There are, however, some issues that many carers share. Carers are more likely than the rest of the population to be affected by health problems such as depression, stress related illness or back pain caused by moving or lifting the person they care for. Carers and the people they look after are also more likely to be on a low income. Many carers combine working with caring, with some caring for more than 50 hours on top of working full time: while others may give up work or reduce their hours because of their caring responsibilities.
Surrey Carers Strategy 2021 to 2024 (extended to 2026) sets out our commitment and determination to help carers continue caring if they are willing and able, and to support their health and wellbeing by achieving outcomes they have identified matter most to them.
From April 2022 new contracts will be in place to ensure that Carers of all backgrounds have timely access to the care and support that they need to maintain their own health and wellbeing as well as that of the people they provide care and support for. Feedback from stakeholders, including carers themselves, during the development of the strategy suggested that access to support for carers of people with disabilities, particularly working age adults, needs to be improved. This feedback informed the specifications for the new contracts and the Carers Dashboard that is currently in its final draft form will demonstrate performance against this target.
We will: Ensure carers of disabled people have access to the support they need to protect their own health and wellbeing as well as that of the person they provide care and support for.
We will: We recognise that they are expert partners in care and will ensure mechanisms are in place for them to make their views known and ensure they are built into co-production activity.
Section 6. Strategy Action Plan
An action plan will be developed to support the delivery of the outcomes of this strategy. This will be co-produced by June 2022.
We will: Hold a Strategy Action Plan Review event once a year with the engagement and input from the whole system to review progress on the Strategy Action Plan and make sure is updated for future years.
Section 7. Developing an infrastructure to implement change
The implementation of the strategy action plan will be overseen by core members of the Physical Disability and Sensory Impairment Steering Group (PDSI SG). The PDSI Steering group will focus on maximising the opportunities for co-production, joint working, and coordination with the user forums and partners across the health, social care, voluntary, community and faith sectors to deliver the action plan outcomes. As living documents, the strategy and action plan should be flexible enough to enable the steering group to respond to opportunities as they arise over the 5 year period of the strategy.
We will: Establish a new governance structure, co-produced with disabled people, to ensure disabled people are part of discussions about how plans for actions creating better opportunities and outcomes are developed and reviewed.
Section 8. Appendices
- Appendix 1: Surrey Prevalence Figures snapshot for 2022
- Appendix 2: Glossary of Terms
- Benefits
- Blue Badges
- Certification and registration
- Children and young people
- Co-production
- Disability
- Disabled people
- Dual sensory loss
- Hearing impairment
- Impairment
- Long-term neurological conditions
- Neuro-disability
- Older people
- Sight loss
- Sight threatening eye conditions
- Social model of disability
- Working age adults
- Unpaid carers
- Appendix 3: Engagement
- Appendix 4: Related Strategies and Further Reading
Appendix 1: Surrey Prevalence Figures snapshot for 2021
- Table 1. Parkinson's in Surrey
- Motor Neurone Disease
- Table 2. Multiple Sclerosis in Surrey
- Sight and Hearing Loss, including D/deafened
Table 1. Estimated number of people diagnosed with Parkinson's in Surrey
| District and borough | Estimated number of people diagnosed with Parkinson's | Estimated number of people over 45 newly diagnosed each year | Surrey total population |
|---|---|---|---|
| Elmbridge | 307 | 38 | 136,626 |
| Epsom and Ewell | 179 | 22 | 79,928 |
| Guildford | 306 | 38 | 147,889 |
| Mole Valley | 251 | 32 | 87,253 |
| Reigate and Banstead | 331 | 41 | 147,757 |
| Runnymede | 190 | 23 | 88,000 |
| Spelthorne | 234 | 30 | 99,334 |
| Surrey Heath | 212 | 26 | 88,874 |
| Tandridge | 220 | 28 | 87,496 |
| Waverley | 338 | 42 | 125,610 |
| Woking | 214 | 26 | 101,167 |
| Total population of Surrey | 2782 | 346 | 1,189,934 |
Source: Parkinson's Society 2021
These are estimates based on the known prevalence rates for Parkinson's and local populations. Overall, we estimate that there is 2% growth per year so by 2027 we'd estimate that there will be over 3000 people living with Parkinson's in Surrey.
Motor Neurone Disease
Surrey has an expected prevalence of around 83 people diagnosed with Motor Neurone Disease based on the national average per population (last recorded statistics.)
The Motor Neurone Disease Association has 141 people living in Surrey diagnosed with MND currently registered with Motor Neurone Disease Association (MNDA). This is a voluntary registration and not based on NHS data therefore the true number of MND patients is likely to be higher as not all choose to register with MNDA.
This is a high number of MND diagnosis, and the MNDA suggest the only viable conclusion was the higher numbers of retired people resident in Surrey which may explain some of the data.
Multiple Sclerosis
New data* from Public Health England (PHE) and the MS Society has revealed that the number of people living with multiple sclerosis (MS) in the UK has risen to over 130,000 – that's around 1 in every 500 people.
The new UK MS prevalence figure is over 20% more than previously thought, rising from 109,000 people. The latest research also shows an increase in the incidence of MS, which is the number of people newly diagnosed with MS each year. The number of diagnoses has risen from an estimated 5,000 in 2017 to 6,700.
The number of people living with MS in all 4 of the UK nations has also increased; there are an estimated 15,750 people living with MS in Scotland, 5,600 in Wales, 105,450 in England and 4,830 in Northern Ireland.
(*The estimate was calculated using 2018 patient information from a general practitioner database).
Table 2. Breakdown of the number of people living with MS in Surrey broken down by Clinical Commissioning Group
| Age | <30 | 30 to 34 | 35 to 39 | 40 to 44 | 45 to 49 | 50 to 54 | 55 to 59 | 60 to 64 | 65 to 69 | 70 to 74 | 75+ | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| NHS Surrey Heath Clinical Commissioning Group (CCG) | <10 | <10 | 12 | 17 | 21 | 29 | 27 | 20 | 21 | 18 | 17 | 194 |
| NHS East Surrey CCG | 11 | 13 | 25 | 33 | 39 | 54 | 49 | 37 | 39 | 32 | 31 | 362 |
| NHS North West Surrey CCG | 21 | 24 | 47 | 63 | 72 | 101 | 93 | 68 | 70 | 58 | 59 | 677 |
| NHS Surrey Downs CCG | 17 | 16 | 34 | 51 | 63 | 90 | 84 | 63 | 66 | 58 | 56 | 597 |
| NHS Guildford and Waverley CCG | 14 | 13 | 23 | 33 | 41 | 56 | 52 | 41 | 43 | 37 | 37 | 390 |
Surrey total: 2220
Source: MS Society 2021
Sight and hearing loss, including D/deafened
- 1 in 6 of the UK adult population is affected by hearing loss.
- 8 million of these are aged 60 and over.
- 6.7 million could benefit from hearing aids but only about 2 million people use them.
- About 900,000 people are severely or profoundly deaf.
- There are an estimated 151,00 people using British Sign Language in the UK, and 87,000 are Deaf. (This figure does not include professional BSL users, interpreters, or translators – Source: British Deaf Association).
This is reflected n The Annual Population Survey (Office for National Statistics) that measures personal wellbeing, asking people to evaluate, on a scale of 0 to 10, how satisfied they are with their life overall, whether they feel they have meaning and purpose in their life, and about their emotions (happiness and anxiety) during a particular period. Data shown here is from the year ending June 2020.
On average, disabled people aged 16 to 64 years had significantly poorer ratings than non-disabled people on all 4 personal wellbeing measures, with the greatest disparity in average anxiety levels.
In the year ending June 2020, the mean scores on these measures were:
- for happiness yesterday, 6.46 out of 10 for disabled people, compared with 7.58 for non-disabled people
- for feeling that the things done in life are worthwhile, 7.06 out of 10 for disabled people, compared with 7.98 for non-disabled people
- for life satisfaction, 6.62 out of 10 for disabled people, compared with 7.81 for non-disabled people
- for anxiety yesterday, 4.47 out of 10 for disabled people, compared with 2.91 for non-disabled people (higher numbers equate to poorer wellbeing in this measure)
Appendix 2: Glossary of Terms
- benefits
- Blue Badges
- certification and registration
- children and young people
- co-production
- disability
- disabled people
- dual sensory loss
- hearing impairment
- impairment
- long-term neurological conditions
- neuro-disability
- older people
- sight loss
- sight threatening eye conditions
- social model of disability
- working age adults
- unpaid carers
Benefits
Disability Living Allowance (DLA) and Personal Independence Payment (PIP) are benefits paid to help people with the extra costs incurred as a result of a disability, and they are paid at different rates depending on the level of need. All working age DLA claimants are having their needs re-assessed, and potentially moved onto PIP in the future.
Blue Badges
Blue Badges are parking badges for disabled people. Local authorities issue them to individuals and organisations concerned with the care of disabled people. Upon issue, a Blue Badge is valid for a period of 3 years. People who are registered as blind are automatically entitled to a blue badge if they register for one (like there will be no further assessment of need as with many other applicants).
Certification and registration
A Certification of Vision Impairment (CVI) formally certifies a person as either sight impaired (partially sighted) or severely sight impaired (blind). A CVI can only be completed by a consultant ophthalmologist. Once complete, copies are shared with (i) the patient, (ii) Moorfields eye hospital (where the record of CVIs is maintained) and (iii) the local social services team, providing a formal route into social care services for the patient.
Registration as blind or partially sighted is voluntary, however it can lead to some benefits and concessions such as blind person's tax allowance, access to loan equipment and help with the cost of travel. Some benefits are automatic whilst others must be applied for.
Children and young people
Children and young people living with a disability based on the age bands: 0 to 17 years and 17 to 25 years.
Co-production
Co-production is an approach to decision-making and service design rather than a specific method. It stems from the recognition that if organisations are to deliver successful services, they must understand the needs of their users and engage them closely in the design and delivery of those services.
Co-production rejects the traditional understanding of service users as dependents of public services, and instead redefines the service/ user relationship as one of co-dependency and collaboration. Just like users need the support from public services, so service providers need the insights and expertise of its users in order to make the right decisions and build effective services.
Disability
A person is considered disabled if they have a self-reported long-standing illness, condition or impairment, which causes difficulty with day-to-day activities. This definition is consistent with the Equality Act 2010 and the Government Statistical Service (GSS) harmonised definition.
Disabled people
Throughout the strategy and Action Plan where the terms "disabled people" or "people with disabilities" are referred to, this should be interpreted as including people with a physical, communication, sensory, general, and / or neuro-disability* including acquired brain injury.
Dual sensory loss
Dual sensory loss is a combination of sight and hearing loss and people with the condition are often also described as deafblind, multi-sensory impaired or dual-sensory impaired. A person is regarded as deafblind if their combined sight and hearing impairment cause difficulties with communication, access to information and mobility. This includes people with a progressive sight and hearing loss.
Hearing impairment
Hearing impairment is measured by finding the quietest sounds someone can hear using tones with different frequencies. Hearing thresholds are measured in decibels hearing levels (dBHL). Anyone with thresholds between 0 and 20 dBHL across all the frequencies is considered to have 'normal' hearing. The greater the threshold level is in dBHL the worse the hearing loss.
Moderate hearing impairment: The quietest sounds that can be heard in the better ear is on average between 35 and 49 decibels.
Severe deafness hearing impairment: The quietest sounds that can heard in the better ear is on average between 50 and 94 decibels.
Profound deafness hearing impairment: The quietest sounds that can be heard in the better ear is on average 95 decibels or more.
Impairment
An impairment refers to health conditions affecting any of the following areas:
- vision (for example, blindness or partial sight)
- hearing (for example, deafness or partial hearing)
- mobility (for example, walking short distances or climbing stairs)
- dexterity (for example, lifting and carrying objects or using a keyboard)
- learning, understanding or concentrating
- memory
- mental health
- stamina, breathing or fatigue
- socially or behaviourally (for example, associated with autism, attention deficit disorder or Asperger's syndrome)
- other
(Source: Government Statistical Service Impairment Harmonisation Standard, May 2020)
Long-term neurological conditions
These can be broadly categorised as follows:
- sudden onset conditions, for example acquired brain injury or spinal cord injury, followed by a partial recovery. (Note: stroke for all ages is covered by Older People)
- intermittent and unpredictable conditions, for example epilepsy, certain types of headache or early multiple sclerosis, where relapses and remissions lead to marked variation in the care needed
- progressive conditions, for example motor neurone disease, Parkinson's disease or later stages of multiple sclerosis, where progressive rapid deterioration in neurological function leads to increasing dependence on help and care from others.
- stable neurological conditions, but with changing needs due to development or ageing, for example Post-polio Syndrome or Cerebral Palsy in adults.
Neuro-disability
The term "neuro-disability" includes the range of disabilities such as Acquired Brain Injury, Multiple Sclerosis, Parkinson's Disease and congenital and childhood conditions such as Cerebral Palsy, Muscular Dystrophy and Spina-Bifida and other rare conditions such as Motor Neurone Disease, Huntington's Disease and Progressive Supra-nuclear Palsy. (This is not an exhaustive list).
Older people
Older people living with a disability based on the age bands: 65 to 74 years; 75 to 84 years; and 85 years and over.
Sight loss
The 3 categories of severity of sight loss are included in this strategy and are taken from the "Future Sight Loss UK 1" report. They are as follows:
- severe sight loss (blindness) is defined as best-corrected visual acuity of <6/60 in the better-seeing eye
- moderate sight loss (partial sight) is defined as best-corrected visual acuity of <6/18 but better than or equal to 6/60 in the better-seeing eye
- mild sight loss (partial sight) is defined as best-corrected visual acuity of <6/12 but better than or equal to 6/18 in the better-seeing eye
These definitions differ from those used in the Certification of Vision Impairment process. Further details about the methodology used to calculate this data can be found in the "Future Sight Loss UK 1" report (Access Economics, 2009). For comparison, further details on the definitions used in the certification process can be found in the "Certification and Registration Processes" report (Boyce, 2012).
Sight threatening eye conditions
There are a number of people who are living with a sight threatening eye condition, or in some cases a number of different sight threatening eye conditions. This includes people who have experienced sight loss as a result of age-related macular degeneration (AMD), cataract, glaucoma and diabetic retinopathy. It also includes people with the early stages of these diseases who have not experienced any reduction in their vision at this point.
Social model of disability
The social model of disability is a way of viewing the world, developed by disabled people.
The model says that people are disabled by barriers in society, not by their impairment or difference. Barriers can be physical, like buildings not having accessible toilets. Or they can be caused by people's attitudes to difference, like assuming disabled people can't do certain things. The social model helps us recognise barriers that make life harder for disabled people. Removing these barriers creates equality and offers disabled people more independence, choice and control.
Working age adults
Working age people living with a disability based on the age band: 18 to 64 years.
Unpaid carers
A person providing unpaid care to another person.
Appendix 3: Engagement
Resident engagement
During our initial engagement phase (November 2020 to January 2021) we launched an initial survey to gather the main thoughts, views and concerns from residents with a physical disability and/or sensory impairment, which generated 73 individual responses. We also produced the survey in a number of accessible formats including Easy Read, Braille and Screen Reader Accessible. We shared the survey with a large range of partners including Sight for Surrey, Action for Carers, Surrey Choice and Health professionals.
We also engaged with a various specific interest groups including all of the Disabled Empowerment Networks, Surrey Vision Action Group, Long-Term Neurological Conditions Group and the Hard of Hearing Forum which resulted in engaging with more than 111 residents.
The insight gained from the survey and through our continued engagement with these groups has resulted in the development of our draft strategy. However, we will continue to engage with these groups and those who responded to our initial survey through invitations to engagement meetings to co-produce the strategy. We are also engaged with a small group of 18 to 24 year olds with a Physical Disability and/or Sensory Impairment via ATLAS to ensure that their needs are also captured. These groups are now helping us to develop the action plan which will support the on-going delivery of the strategy.
Staff engagement
We held 6 engagement sessions for staff within our locality and transitions teams, including Occupational Therapists and social workers. We had over fifty attendees in total to the 6 sessions held.
Appendix 4: Related strategies and further reading
This Strategy should be read in conjunction with the related strategies below:
- Surrey Adult Social Care Accommodation with Care and Support Strategy
- Surrey Carers Strategy 2021 to 2024
- Family Resources Survey (2019 to 20)
- Surrey's Health and Wellbeing strategy
- Labour Force Survey (LFS)
- Labour market status of disabled people datasets
- The Physical Activity Strategy 'Movement for Change (Active Surrey)'
Easy Read alternative (PDF)
Download a Easy Read (PDF) version of the Adult Social Care Strategy for people with Physical Disability and Sensory Impairment (PDSI).